Lyme Disease
 Lyme disease is a bacterial infection caused by an infected tick. It is most common in the United States, especially in the Northeastern, mid-Atlantic, Midwest, and Pacific coast; in Canada, notably in central and southeastern regions; and in Europe. As the infection spreads in ticks and people become more mobile, the areas of caution for Lyme disease continue to expand.
Lyme disease is a bacterial infection caused by an infected tick. It is most common in the United States, especially in the Northeastern, mid-Atlantic, Midwest, and Pacific coast; in Canada, notably in central and southeastern regions; and in Europe. As the infection spreads in ticks and people become more mobile, the areas of caution for Lyme disease continue to expand.
Ticks thrive in forested areas but can live anywhere, including your yard. Ticks become infected with the transfer of bacteria as they feed off deer and rodents. When the tick enters a human’s skin to feed, it places the bacteria in the human’s bloodstream. If the tick is not found on the human, it can feed for several days, swelling as it ingests blood. The same process can occur when spreading the disease to other animals, including your pets.
In the United States, the most common tick that carries the infection in the Northeast and Midwest is the black-legged deer tick. In the West, the most common carrier is the western black-legged tick. Not all ticks are infected. Only ticks that are infected spread the bacteria. More types of ticks are being identified as carriers of infectious diseases including Lyme disease. The bacteria that cause Lyme disease include Borrelia afzelii, Borrelia garinii, Borrelia mayonii, and Borrelia burgdorferi with more types being discovered.
The black-legged deer tick (ixodes scapularis). Adult ticks can be as large as a quarter of an inch, young ticks are less than one-eighth of an inch making them difficult to see.
Lyme disease can occur at any time. Outdoor temperature affects the rate of spread with spring summer and fall being the highest time of reported cases. April through October is the height of the tick season in the U.S. However, any time the temperature is above freezing, ticks are active. Ticks can be anywhere but particularly thrive in woods, shrubs, or grassy spaces. Ticks can even be in your yard. Certain areas of continents have higher rates of the spread of Lyme disease but as people, animals, and ticks are mobile, these areas are expanding.
Areas of Lyme disease prevalence are noted on the map below. In the U.S., the Centers for Disease Control and Prevention (CDC) publishes this interactive map to illustrate the areas where Lyme disease is most prominent.
Prevention is always the best way to avoid chronic disease. Tips to prevent Lyme disease include:
- Use Environmental Protection Agency (EPA)-approved tick repellent as directed and age-appropriate. Include clothing, shoes, tents, and lawn chairs.
- Wear long pants tucked into your socks and long-sleeved shirts tucked into your pants.
- Wear fully enclosed shoes.
- Visualize ticks more easily by wearing light-colored clothing.
- When outside, stay on cleared paths, avoiding wooded, bushy, and grassy areas.
- Remove clothing worn outdoors as soon as you come inside and place them in a dryer for 10 minutes to kill ticks before washing clothing.
- Shower as soon as coming indoors to wash ticks that may be on your body but not yet burrowed.
- Check your body and your children’s body for burrowed ticks and tick bites.
- Use a mirror to check areas of your body that you cannot view easily.
- Carefully examine hairy areas, ears, and bellybutton.
- Check your pets for ticks and tick bites.
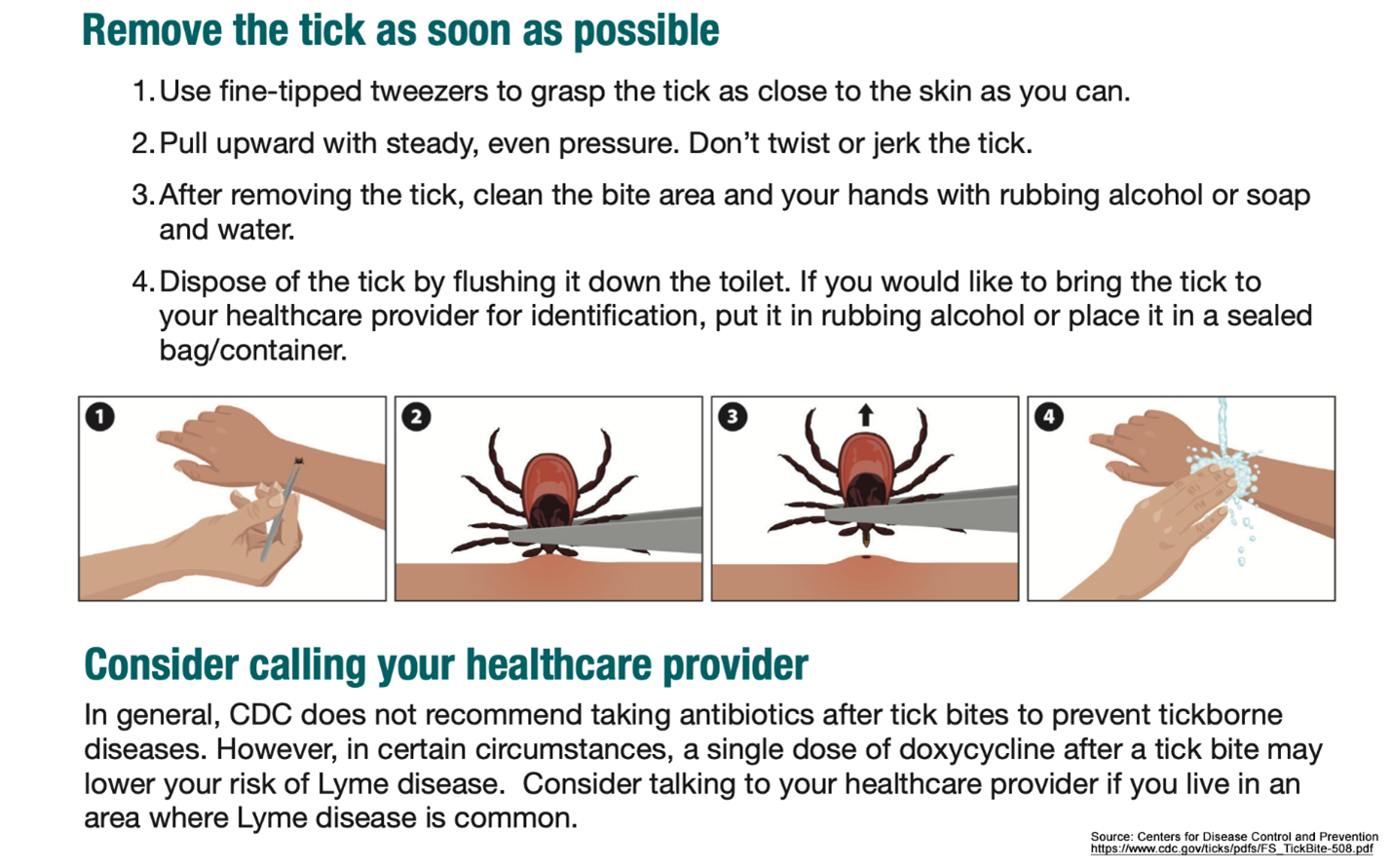
Lyme disease does not result from every tick bite. Only the bite of an infected tick will transmit the disease. The tick must be attached for 12 to 24 hours before it can spread the disease. Prompt removal of the tick is critical to avoiding Lyme disease. Avoid various tales about tick removal. The CDC recommends these guidelines for prompt and safe tick removal.
Symptoms/Diagnosis
Symptoms of Lyme disease can be different for each person. Often individuals do not have any immediate symptoms of Lyme disease or notice that they had a tick bite. Some individuals may have an itchy bump on their skin that looks like an average bug bite.
The consequences of Lyme disease can range from no issues to severe effects. Some cases result in rashes, fever, and fatigue. In severe cases, multiple organs of the body are affected resulting in chronic health issues.
In January 2024, one case of Lyme disease was associated with the development of transverse myelitis (TM). Although the development of TM is rare, it is one example of a neurological complication. If you already have neurological or other health issues, Lyme disease could affect your pre-existing condition.
Early symptoms of Lyme disease may include no symptoms or a red rash of varying intensity and duration. It can look like other rash types or even sunburn. The area may feel warmer than the rest of the skin. It can disappear and return even weeks later.
The classic rash of Lyme disease looks like a ‘bullseye’ on the skin that can expand over time. Depending on the duration of the infection, this rash can be extremely faint to a large, red shape. It can appear anywhere on the body where the tick bite occurred.
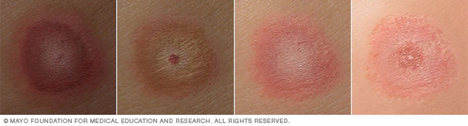
Illustration of Lyme disease rash on different skin tones. People with Lyme disease might have a ‘bull’s-eye’ rash. The bull’s-eye rash gradually spreads over days.
Photo Credit: Used with permission of Mayo Foundation for Medical Education and Research, all rights reserved.
Midterm Symptoms may develop days or weeks after infection and appear ‘flu-like’, These symptoms mimic other common illnesses which make diagnosis more challenging especially if there was no known tick bite or bull’s-eye rash. The midterm symptoms may include all or just some of the following:
- Headache
- Stiff neck
- Joint pain
- Low-grade fever/chills
- Tiredness
- Poor appetite
- Swollen glands
Late-Term Symptoms can develop over weeks to months or years later.
Weeks to months:
- Nervous system inflammation
- Facial muscle weakness or paralysis (Bell’s palsy)
- Heart inflammation (myocarditis)
- Heart rate changes
- Eye problems and inflammation (red eye)
Months to years:
- Arthritis, inflammation of joints
- Numbness, tingling, pain in extremities
- Speech difficulty
- Memory loss
- Concentration issues
Post-Lyme Disease Syndrome (PLDS) can occur as a chronic disease. This includes persistent issues of musculoskeletal issues, peripheral nerve pain, fatigue, and memory concerns.
Diagnosis
Your healthcare provider will ask questions about your symptoms, including when they first appeared. They will want to know if you have had a tick bite. If you know you did, show them the area. A complete skin examination may be performed if you know of a tick bite or are unaware of one. Since Lyme disease symptoms are the same as many other common health issues, they will ask about your exposure to other diseases.
Recognizing the bull’s-eye rash is key to diagnosis. However, most cases do not have this presentation which makes diagnosis challenging. A healthcare professional with experience diagnosing Lyme disease may be more proficient in recognizing the issue. If you think you may have Lyme disease, mention it in your appointment with your healthcare provider to bring the issue into the conversation.
A standardized two-tier blood test is recommended for Lyme disease diagnosis. A blood sample is taken from your arm with a needle as with any blood test. Once your blood specimen is obtained, the sample is evaluated in a laboratory.
- The first analysis of the blood is an enzyme immunoassay (EIA) also known as an enzyme-linked immunosorbent assay (ELISA) (a measurement of antibodies, antigens, proteins, and hormones in the blood) OR immunofluorescent assay (IFA) (use of fluorescence to determine the presence of antibodies that react with antigenic material.) One of these tests is performed to avoid false positive results.
- The second analysis of your blood sample is a Western blot test. This test will note specific proteins of Lyme disease. These are tests to see if your body is fighting Lyme disease bacteria, meaning it is present in your body.
If you suspect you may have Lyme disease, some blood drawing laboratories will provide a blood test without a physician’s order at your own cost. The tests may not be the correct assessment for Lyme disease. Be sure you are working with a healthcare provider to get the appropriate testing which requires a healthcare professional’s order.
Co-Infection
Ticks often carry more than one bacterium at a time. Therefore, you can have a co-infection. The symptoms of tick co-infections are frequently the same as Lyme disease. Common tick co-infections include:
- Anaplasmosis is the most frequent co-infection with Lyme disease in 10% of cases. It is also a bacterial infection but from the bacteria, Anaplasma phagocytophilum. Symptoms include fever, chills, headaches, and muscle aches. It appears 1-2 weeks after the tick bite.
Rarely:
- Babesiosis is a parasite carried by ticks infected with Lyme disease. Some individuals have no symptoms, others may have flu-like symptoms. This parasite destroys red blood cells leading to anemia. It can be life-threatening for individuals with compromised immune systems (as with neurological injury), over the age of 50, liver, or kidney disease (as with diabetes), or with a removed or poorly functioning spleen.
- Powassan virus is rare but increasing and is transmitted by tick bites. Symptoms are flu-like and can lead to brain and spinal cord infections.
- Hard tick relapsing fever (HTRF) is caused by a bacterium that can occur with Lyme disease tick bites. Symptoms include chills, fatigue, nausea/vomiting, headache, and joint or muscle aches. Most individuals recover without treatment. It is more severe in those individuals who are immunocompromised.
Treatments
An antibiotic is the primary treatment for Lyme disease, including the co-infections of anaplasmosis and hard tick relapsing fever. Babesiosis typically does not require treatment. The Powassan virus does not yet have a treatment. Your healthcare professional will determine the correct antibiotic for you based on your health condition and history.
The earlier treatment with antibiotics begins, the better the results. It may be given as a precaution if a tick bite occurs in an area with known Lyme disease, even before blood tests are performed. The usual course of antibiotic treatment is 14 to 21 days. Those with Lyme arthritis should receive antibiotics for 28 days. If the disease is diagnosed later, three to four weeks of antibiotics may be required. Individuals with neurological symptoms should have antibiotics given by IV.
Lyme disease, anaplasmosis, and hard tick relapsing fever treatment of choice include mainly these antibiotics:
- Doxycycline prevents the spread and growth of bacteria. It is a member of the tetracycline antibiotic group.
- Amoxicillin is a penicillin type of antibiotic but has an added amino group to its formulation reducing the bacteria’s survival.
- Cefuroxime axetil disrupts the cell wall formation of bacteria, reducing the survival of the bacteria.
- Azithromycin inhibits protein synthesis causing an inability of the germ to survive.
Antibiotics must be taken for the full course of treatment. After a few doses, you may feel better, but the bacteria are still in your body. If the full course of antibiotic treatment is interrupted, the bacteria will become stronger. This will make further treatment more difficult and may lead to post-Lyme disease syndrome. Take the complete course of antibiotics to destroy the bacteria and to avoid complications.
Rehabilitation Therapies
Treatments for Lyme disease begin with the precautions taken to avoid it. Most individuals will recover from Lyme disease within two to four weeks with antibiotic treatment. A smaller number of individuals may have long-term complications.
Your healthcare professionals will tell you about actions to take to maintain your health. Maintain good health practices by getting rest, light exercise, hydration, and healthy eating. Antibiotics can affect the digestive tract. If your healthcare professional recommends a probiotic, add that to your routine, but only for the time recommended.
Long-term issues of Lyme disease can become chronic concerns. Specialists will assist with guiding treatments:
Nervous system inflammation, headache, numbness, tingling, weakness, and paralysis will be treated by a neurologist who will recommend physical, occupational, and speech therapies as needed. These treatments may include strengthening exercises, mobility equipment, and pain and tone (spasticity) management.
Cardiac system issues such as inflammation of the heart, heart rate changes (pulse too fast or too slow), or heart contractions will be treated by a cardiologist. Diagnostic procedures such as EKG (electrocardiogram), echocardiogram (ultrasound of the heart), stress test, or cardiac catheterization may be performed with the appropriate treatment and recommendations. These may include medication or a pacemaker among others.
Eye problems and inflammation may be due to bacteria or nerve issues specifically in the eyes. An ophthalmologist will be able to prescribe the correct treatment for you to resolve or improve visual issues. This may include glasses or other corrective procedures such as eye exercises or surgical corrections.
Inflammation of joints may result in arthritis which is treated by a rheumatologist. Treatments may include medications to reduce inflammation and therapies to help conserve energy and reduce pain.
Individuals with speech difficulties may be referred to a speech and language pathologist who will provide therapies for retraining muscles to help form words, improve speech, and assist with swallowing difficulties.
Memory loss and concentration issues are generally treated by a neurologist or psychologist who will offer strategies to improve memory function. Some individuals may receive medication to enhance brain function or strategies for coping with memory issues.
Fatigue is an issue that can be found in any of the above health issues. Physical and occupational therapists can provide treatment strategies to conserve energy and slowly rebuild tolerance.
Dealing with a chronic disease can be challenging for an individual and their family. A psychologist can assist with the development of methods to help cope with these obstacles.
History
The first case of Lyme disease was reported in Lyme, Connecticut in 1975. There were scant publications about it until 1984. As this is a relatively newly recognized condition, prevention strategies and treatments are still being developed and studied.
A vaccine was developed for Lyme disease but was discontinued in 2002 due to a lack of consumer demand. If you received this vaccine before 2002, its efficacy has decreased. Most likely, you are no longer protected. Continued work on a longer-lasting vaccine for Lyme disease is in development. A vaccine for the co-infection, Powassan, is being developed for treatment.
As Lyme disease spreads quickly, education about rash, fever, fatigue, and treatment is becoming more prevalent in healthcare and the public. The eradication of Lyme disease at the source is being researched.
Clinical trials are being conducted to gain more information about progression, treatment, and recovery. If you choose to participate in a clinical trial (research study) of Lyme disease, search for clinical trials on the website.
Facts and Figures
In the United States, between 63,000 and 450,000 cases of Lyme disease are reported annually depending on the data collection method. Estimates of over 3 million annual cases are diagnosed worldwide.
In 1991, Lyme disease became a condition required to be reported to the local and state health departments in the U.S.
Lyme disease can develop in anyone regardless of background if infected by a tick carrying the disease. Pets can also have Lyme disease. There are higher incidences in areas where ticks are more prominent.
Ticks need to be attached for 12-24 hours before Lyme disease can spread to the host.
May is Lyme disease awareness month. The awareness ribbon is lime green.
Resources
If you are looking for more information about Lyme disease or have a specific question, connect with our Information Specialists.
Additionally, the Reeve Foundation maintains fact sheets with additional resources. Check out our repository of fact sheets on hundreds of topics ranging from state resources to secondary complications of paralysis.
We encourage you to reach out to organizations, including associations that feature news, research support, resources, national networks of support groups, clinics, and specialty hospitals.
Community Resources
American Lyme Disease Foundation
Centers for Disease Control and Prevention (CDC)
International Lyme and Associated Diseases Society
Clinical Guidelines
American Academy of Family Physicians Update
Infectious Diseases Society of America (IDSA), American Academy of Neurology (AAN), and American College of Rheumatology (ACR): 2020 Guidelines for the Prevention, Diagnosis, and Treatment of Lyme Disease
References
Błaut-Jurkowska J, Jurkowski M. Borelioza–aktualny stan wiedzy [Lyme Disease–An Update]. Przegl Lek. 2015;72(11):656-61. Polish. PMID: 27012125.
Bockenstedt LK, Wormser GP. Review: Unraveling Lyme Disease. Arthritis Rheumatol. 2014 Sep;66(9):2313-23. doi: 10.1002/art.38756. PMID: 24965960; PMCID: PMC4282157.
Carriveau A, Poole H, Thomas A. Lyme Disease. Nurs Clin North Am. 2019 Jun;54(2):261-275. doi: 10.1016/j.cnur.2019.02.003. Epub 2019 Mar 26. PMID: 31027665.
Coderre-Ball AM, Sahi S, Anthonio V, Roberston M, Egan R. Lyme Disease Training and Knowledge Translation Resources Available to Canadian Healthcare Professionals: A Gray Literature Review. J Prim Care Community Health. 2021 Jan-Dec;12:21501327211050744. doi: 10.1177/21501327211050744. PMID: 34654327; PMCID: PMC8521418.
Coiffier G, Tattevin P. Lyme Disease: “End of the Debate?”. Joint Bone Spine. 2021 Jul;88(4):105181. doi: 10.1016/j.jbspin.2021.105181. Epub 2021 Apr 1. PMID: 33812988.
Donta ST. What We Know and Don’t Know About Lyme Disease. Front Public Health. 2022 Jan 21;9:819541. doi: 10.3389/fpubh.2021.819541. PMID: 35127630; PMCID: PMC8813852.
Dumes AA. Lyme Disease and the Epistemic Tensions of “Medically Unexplained Illnesses”. Med Anthropol. 2020 Aug-Sep;39(6):441-456. doi: 10.1080/01459740.2019.1670175. Epub 2019 Dec 20. PMID: 31860363.
DuPrey KM. Lyme Disease in Athletes. Curr Sports Med Rep. 2015 Jan;14(1):51-5. doi: 10.1249/JSR.0000000000000118. PMID: 25574885.
Eckenrode K. Early Identification of Lyme Disease Complications. JAAPA. 2023 Jan 1;36(1):19-23. doi: 10.1097/01.JAA.0000902892.41571.17. PMID: 36573811.
Evans J. Lyme disease. Curr Opin Rheumatol. 1995 Jul;7(4):322-8. doi: 10.1097/00002281-199507000-00010. PMID: 7547110.
Forrester JD, Vakkalanka JP, Holstege CP, Mead PS. Lyme Disease: What the Wilderness Provider Needs to Know. Wilderness Environ Med. 2015 Dec;26(4):555-64. doi: 10.1016/j.wem.2015.05.001. Epub 2015 Jul 2. PMID: 26141918.
Higgs S, Brissette CA. An Overview of Lyme Disease in Europe. Vector Borne Zoonotic Dis. 2023 Apr;23(4):137-138. doi: 10.1089/vbz.2023.29006.hig. PMID: 37071409.
Izac JR, Marconi RT. Diversity of the Lyme Disease Spirochetes and its Influence on Immune Responses to Infection and Vaccination. Vet Clin North Am Small Anim Pract. 2019 Jul;49(4):671-686. doi: 10.1016/j.cvsm.2019.02.007. Epub 2019 Apr 6. PMID: 30967254; PMCID: PMC6510272.
Mac S, da Silva SR, Sander B. The Economic Burden of Lyme Disease and the Cost-Effectiveness of Lyme Disease Interventions: A Scoping Review. PLoS One. 2019 Jan 4;14(1):e0210280. doi: 10.1371/journal.pone.0210280. PMID: 30608986; PMCID: PMC6319811.
Marchese NM, Primer SR. Targeting Lyme Disease. Nursing. 2013 May;43(5):28-33; quiz 33-4. doi: 10.1097/01.NURSE.0000428691.49098.16. PMID: 23542090.
Marques AR. Lyme Disease: A Review. Curr Allergy Asthma Rep. 2010 Jan;10(1):13-20. doi: 10.1007/s11882-009-0077-3. PMID: 20425509.
McCarthy CA, Helis JA, Daikh BE. Lyme Disease in Children. Infect Dis Clin North Am. 2022 Sep;36(3):593-603. doi: 10.1016/j.idc.2022.03.002. PMID: 36116837.
Mustafiz F, Moeller J, Kuvaldina M, Bennett C, Fallon BA. Persistent Symptoms, Lyme Disease, and Prior Trauma. J Nerv Ment Dis. 2022 May 1;210(5):359-364. doi: 10.1097/NMD.0000000000001452. PMID: 35413029.
Mushtaq A, Kazi F. New Guidelines for Lyme Disease Diagnosis. Lancet Infect Dis. 2021 Feb;21(2):173. doi: 10.1016/S1473-3099(21)00009-8. PMID: 33515521.
Randolph SA. Lyme Disease. Workplace Health Saf. 2016 Jan;64(1):40. doi: 10.1177/2165079915616398. Epub 2015 Nov 19. PMID: 26585171.
Ross Russell AL, Dryden MS, Pinto AA, Lovett JK. Lyme Disease: Diagnosis and Management. Pract Neurol. 2018 Dec;18(6):455-464. doi: 10.1136/practneurol-2018-001998. Epub 2018 Oct 3. PMID: 30282764.
Schmid H, Heininger U. Posttreatment Lyme Disease Syndrome–What It Might Be and What It Is Not. Pediatr Infect Dis J. 2021 May 1;40(5S):S31-S34. doi: 10.1097/INF.0000000000002772. PMID: 34042908.
Schoen RT. Challenges in the Diagnosis and Treatment of Lyme Disease. Curr Rheumatol Rep. 2020 Jan 7;22(1):3. doi: 10.1007/s11926-019-0857-2. PMID: 31912251.
Shapiro ED. Lyme Disease. Adv Exp Med Biol. 2008;609:185-95. doi: 10.1007/978-0-387-73960-1_14. PMID: 18193666.
Shapiro ED, Gerber MA. Lyme Disease. Clin Infect Dis. 2000 Aug;31(2):533-42. doi: 10.1086/313982. Epub 2000 Sep 14. PMID: 10987718.
Shea J. Physical Therapist Recognition and Referral of Individuals With Suspected Lyme Disease. Phys Ther. 2021 Aug 1;101(8):pzab128. doi: 10.1093/ptj/pzab128. PMID: 34003263; PMCID: PMC8389172.
Smith BG, Cruz AI Jr, Milewski MD, Shapiro ED. Lyme Disease and the Orthopaedic Implications of Lyme Arthritis. J Am Acad Orthop Surg. 2011 Feb;19(2):91-100. doi: 10.5435/00124635-201102000-00004. PMID: 21292932; PMCID: PMC3656475.
Sordet C. Chronic Lyme Disease: Fact or Fiction? Joint Bone Spine. 2014 Mar;81(2):110-1. doi: 10.1016/j.jbspin.2013.12.003. Epub 2014 Feb 24. PMID: 24582003.
Stanek G, Strle F. Lyme Disease: European Perspective. Infect Dis Clin North Am. 2008 Jun;22(2):327-39, vii. doi: 10.1016/j.idc.2008.01.001. PMID: 18452805.
Van Hout MC. The Controversies, Challenges and Complexities of Lyme Disease: A Narrative Review. J Pharm Pharm Sci. 2018;21(1):429-436. doi: 10.18433/jpps30254. PMID: 30458921.
Van Solingen RM, Evans J. Lyme disease. Curr Opin Rheumatol. 2001 Jul;13(4):293-9. doi: 10.1097/00002281-200107000-00009. PMID: 11555731.
Wong KH, Shapiro ED, Soffer GK. A Review of Post-Treatment Lyme Disease Syndrome and Chronic Lyme Disease for the Practicing Immunologist. Clin Rev Allergy Immunol. 2022 Feb;62(1):264-271. doi: 10.1007/s12016-021-08906-w. Epub 2021 Oct 23. PMID: 34687445.
